I stumbled upon a PDF recently written awhile back by an anti-vaxxer who gave hilariously god-awful advice on how to debate pro-vaxxers.
His advice:
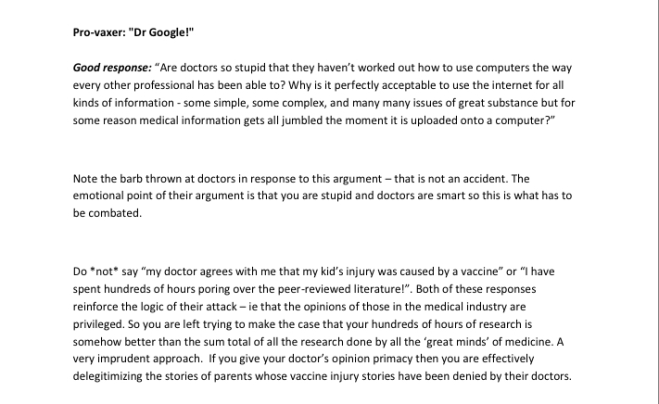
Response: You may want to let them know that nobody out there is insulting anything found on the internet. Not only are you and a majority of doctors a huge fan of computers, but you are more than willing to offer them advice on great online classes to take to help them learn what an argument is. Take this for example:
Pro-vaxer: “glad to see you got your google university degree”
Let’s pretend this is English class. What is the point is the “author” trying to make?
- “All information found online is false”
- “Computers are stupid”
- “Those doctors you’re talking down to for supposedly not ‘doing research’ spent 4 years of undergrad, 4 years of med school, 3 years of residency, and another couple years of a fellowship along with 300K in student loan debt to get where they are today, while you think 4 hours typing VacCinEsKiLlBaBies into your search bar one afternoon compensates for your lack of credentials.
(It’s 3, by the way).
To continue, it’s anti-vaxxers that seem to be “privileged,” considering their demographics are mainly just whiterichmoms in California suburbs. The word they’re thinking of is “expertise,” which is the same reason I don’t fight with computer programmers about how much I hate JavaScript. I don’t sit around angrily explaining to a mechanic that they need to “do research” because they don’t want to do what I watched on Youtube. Even if the person spent “hundreds of hours” researching, big whoop. Still not impressed. 100 hours of “research” gives you one average week of medical school. 100 hours of “research” gives you one week of writing a dissertation. Congrats.
[This was a screenshot from my flashcard deck from only 30 days]


Refutation: Did any of the conversation involve homeopathy, or are they just pulling that assumption out of their ass?
I doubt I have to explain this to anyone, but if an anti-vaxxer starts playing a guessing game of what you don’t personally like that has nothing to do with the argument (e.g “are you an expert on Yugoslavian Yak dancing?? Aha! I got you!”), then they have already lost the argument. I can’t think of much worse advice to give someone than “just use a really obvious red herring- they’ll never notice.”
We will notice.
As if that wasn’t bad enough, “Another good response” then deviates from the subject even further. Not one bit of this response has anything to do with immunology. It’s so awful that I thought I was reading the wrong page at first. I have no idea where on earth they were going with blind trust and responsibility, considering it has nothing to do with expertise in immunology.
And when they respond with “oh by the way, here are a list of immunologists who are opposed to vaccines,” try to hold in the laughter while you explain that it kind of simultaneously negates both their rant on “appeal to popularity” along with the “appeal to authority.” If they backtrack, calmly present the 60,000 immunologists who thank vaccines. If that’s not enough, print out the 148,000 inactive and 44,000 active physicians, grunting things like “who needs trees?” As the piles and piles of paper come out.
Aside from the irony there, be sure to let them know that people in homeopathy or astrology are welcome to write peer review. Nobody is stopping them, and they have done so in the past. Let them know that nobody is angry that you’re “comparing” mere words with each other, as your opinion is based off of evidence, not offense. And then for the love of god, tell them how to stay on one topic.

Refutation: I’m going to guess you never said “but vaccines are science,” considering I’ve never heard that sentence used once, and I’m not sure they have either. It doesn’t even make sense. Maybe they’re missing a couple words.
But in this hypothetical situation, pretending you really did say something that stupid, there’s a very easy one-word response to this.
“Math.”
Math exists, though I wouldn’t be surprised if they also believe math is a government conspiracy. Eugenics, on the other hand, is a personal fucked up belief system, popular among antivaxxers. Math is not. Anti-vaxxers seem to think “science” is literally one subject. It shouldn’t take a genius to figure out why piles of statistically-significant meta-analyses hold more weight than an angry neckbeard screaming racist opinions.
The “dodgy statistics” they’re referring to is a fallacious retort at best. Ask them what they found wrong with them when they checked the math using their R or SPSS program (although I’ll give them credit if they do it cheaper on Excel- whatever works). Let them know that “journal club,” a class/meeting/mini version of hell where scientists get together and judge the shit out of each other’s papers, does this, so they probably should too before making this up and hoping its true. Have the statistics results on hand and ask them what ANOVA they personally prefer, and how they would make it better.
Let them know that Engineers, mechanics, and “some types of medical practitioners” also do not have time machines. Explain to them that research isn’t equivalent to claiming omnipotence. Ask them what on earth they think immunology is, and why they were left out of the fun time and space continuum the rest of us are enjoying. Ask them to explain all of the piles and piles of studies showing efficacy if it’s a myth in immunology.

Refutation: ask them why they’re so obsessed with homeopathy, and if thats who they get their tin foil hat from.
No, don’t do that.
First of all, the Tuskegee syphilis studies were a big fucking deal, considering they were a huge act of genocide against African Americans. If you don’t know what they are, learn. This and the Nazi experiments was something that burgeoned the start of ethical committees being involved in research. I’m honestly stunned (and kind of disgusted) they told people to focus on “mundane” instead, considering the number of people who would have to be involved in something secretive involving vaccines would go far past “mundane.” I have heard the Tuskegee syphilis studies repeatedly in high school, undergrad, and grad school- they were despicable. One can never learn too much about the racism that runs rampant in US history; it’s flowing with it. And I am not remotely surprised that either a white rich soccer mom or uneducated white male wants to deviate from the topic of African Americans never given treatment for syphilis decades after it was available. DECADES. So I’m going to focus on it, since I personally think it’s important to acknowledge institutionalized racism whenever the subject is brought up.
The Tuskegee Syphilis studies are not secret information, and should have been taught in class. African American men were used as the controls for a syphilis study, and treatment was withheld from them even decades after it was shown to work effectively. This meant they died slowly in an excruciating way, as tertiary syphilis affects the brain and CNS, literally degrading brain tissue. These studies are one of the reasons research has to be extremely regulated nowadays because, eventually, some asshole would willingly screw people over again (Donald trump is president, for fucks sake). Even though it’s a pain to go through so much paperwork, I’m thankful it’s done in the long-run, as it keeps someone else from being approved for research that may hurt others.
As for vaccination, this has been going on for decades, and their materials and methods are available for anyone who wants to read them. In order to have a secret government conspiracy going on, you’d have to have every immunology PhD, Pharm.D, immunologist, pediatrician, all nurses in those fields, nurse techs, etc. be in on a giant conspiracy. Considering 1/7 people in the US work in healthcare, the assumption that millions of individuals plus their extended family have been hiding a secret for decades involving secretly administering autism and cancer into children through vaccines is downright laughable. This couldn’t happen, and it makes no sense as to why healthcare workers would get vaccinated themselves if they knew they were so toxic.
Focusing on racism doesn’t somehow simultaneously negate the efficacy of vaccines (another red herring), but I wanted to take a moment to at least acknowledge the genocide that an anti-vaxxer thought was too pointless to mention. Science has absolutely fucked up in the past. Science is not a person. Science is filled with many different individuals spreading over many different fields. But all of these fields today have to get approval from ethical committees before they do any experimentation on humans or animals. It’s a long, tedious process. And if you’re having doubts about pro vaccine research being so unethical that innocent lives are loss (which would be a near impossibility), there should be documentation of their ethics approval and their methods. Anyone who is found to experiment on people without approval, like Andrew Wakefield, will have their paper retracted and most likely lose their job. Most importantly, I have no doubt that racists existed in research in the past, considering they existed everywhere. While I know the writer isn’t from the United States, I am. And anyone who doesn’t know about the Tuskegee Syphilis studies should read more about them.
Response: “okay, so you’re an anti-vaxxer.”
Refutation: “how do you know it will be equivalent to 500 vaccines in 18 months?” This was made up on the spot, as are most anti-vaccine arguments. Vaccines are not equivalent to the value of a dollar – it’s a fucking vaccine. The value doesn’t change over time. Ask them to show you the sources.
While “baby killer” may be a more puerile response, let them know you’re calling them one because they’re actually responsible for babies suffering and dying. They are literally killing babies.
Response: first of all, if you actually said that, you should phrase this differently. The first is a red herring and a pretty stupid argument at that. The question should be rephrased for the point you’re actually trying to make: asking them why they only trust a doctor’s opinions for treatment instead of prevention, and where they draw the line. Research shows that anti-vaxxers are more likely to avoid preventative measures, like annual checkups, and their kids are hospitalized more often because of it. Hilariously enough, this paper was quoted to me by an anti-vaxxer who thought it was “proving” anti-vaxxers are healthier, without realizing that the paper was actually showing that they give no fucks about prevention. Why do they trust doctors for emergencies, many of which are their faults, instead of wanting their child to not get sick in the first place? Why are they okay with parents letting their kids die in front of them?
Also, ask them how nuclear power works. When they stutter, ask why they blindly trust the scientists who support nuclear power, when they obviously don’t know what it is.
Retort: the anti-vaccine movement, thanks to McCarthy, is built upon a foundation trying to eradicate autism, so of course it’s ableist. There are literal websites called “age of autism.” The anti-vaccine movement’s very existence is ableist and degrading. Absolutely, they hate autistic people. I have yet to find a single anti-vaxxer who shows otherwise, and many happily admit this if you ask them about it. I also have yet to find a single autistic individual who doesn’t think the anti-vaccine movement is ableist. Anti-vaxxers don’t care what those who are autistic think. Instead, they will cyberbully them, send them death threats, and speak over them. Anti-vaxxers definitely hate autistic people, and will often say this to your face.
Not to mention, notice how they’re equivocating? There’s a really easy response to those, too. All of those “side effects,” one is way more likely to get if they catch the vaccine-preventable disease. Mumps can cause deafness, polio causes a horrible paralysis that eventually goes to the diaphragm, and rubella is the “R” in ToRCHes infections (it is known for causing congenital defects. I’ve never heard of someone going deaf from MMR (just a mumps infection), and you can’t get a lesser case of polio from the killed polio virus. Rubella is safe to be vaccinated against during pregnancy; they’re thinking of actual rubella. You are WAY more likely to get side effects from the actual diseases- there’s no contest there. Have on hand the piles and piles of statistics supporting this statement. If they actually cared about preventing disability, they’d be pro-vaccine (but they’ve never been too fond of that whole “prevention” thing). Instead, they call their children “injured,” and mourn their very existence. When they’re not calling their children injured failures, they’re mocking anyone else whose autistic. Anti-vaxxers hate autistic people

Refutations: where do I even begin with this one? Here we are reminded that anti-vaxxers literally have no idea what these words mean or how science works.
For the last time: MATH. This should not be a hard concept. I seriously doubt at this point that any anti-vaxxer would pass a 5th grade math class.
We know causation because we are able to show causation. That’s the entire fucking point. You’re not going to get causation from an observational study, the backbone of anti-vaccine research. We’re not going to get causation when we reject the null hypothesis time and time again that vaccination is related to autism diagnoses. We’re also not getting causation from correlation- we have actual evidence of causation between these diseases and their horrible consequences. We have the Germ Theory on our side (which may explain why so many anti-vaxxers reject this scientific theory). We have actual experimental papers supporting the efficacy of current required vaccinations. We have equations accurately predicting the effects of herd immunity.
Math. We have actual math on our side. We are for vaccination because of statistical significance. Anti-vaxxers barely even have the correlation on their side supporting them with the few papers even showing something negative. Their greatest weapon is whatever they make up on the spot.
As for the challenge, dechallenge, rechallenge, you obviously can’t do that with vaccines, and this should be common sense. How can you “dechallenge” long term immunity? You can’t. This isn’t something flushed out of your system like a amphetamines, your body develops antibodies that cannot be “dechallanged.”

Response: Who the fuck has said this? No, the world doesn’t go off of sunshine and bubbles instead of money. But the reason so many of us are huge fans of vaccination is because they are both fiscally responsible and health responsible. When it comes to finances and unscrupulous individuals who may just be in their field for money (which is pretty funny to think about given the amount of student loans and time spent for medical school), vaccines do help the economy by saving money- this isn’t a horrible thing. Some insurance companies even give pediatricians a small amount of money for ensuring the kids are vaccinated. Of course insurance companies aren’t doing everything out of the “goodness of their hearts” or my husband wouldn’t have received health insurance a lot easier with his pre-existing health condition. Instead, they know that paying $400 for an incentive is a lot cheaper than forking out $40,000 for measles encephalitis. The incentive is further evidence that vaccines save lives, and anti-vaxxers somehow don’t see this. It shouldn’t take a rocket scientist to figure out that insurance companies don’t want to pay for someone’s hospital bills. And doctor’s entire job is prevention and treatment of illness. Your health insurance doesn’t care as much, I can promise you that. Again, even the most unscrupulous individual who is only in it for the money would rather avoid getting sued and paying for extra hospital bills. This shouldn’t be a hard concept.
But just in case it is still somehow difficult, a country learned the hard way that avoiding vaccination means losing both money and citizens.
So even though this guy pulled the causation between GDP and vaccination out of his hind quarters, if we agree with him, it still makes his point hilariously backwards by promoting the efficacy of vaccination with the amount of hospital bills avoided for those who are on Medicaid. Regardless, I also wish anti-vaxxers would one day finally realize that the entire world doesn’t revolve around pediatricians. I don’t know why they’re so obsessed with physicians, as if they’ve never heard of PhDs, Pharm.Ds, PAs, LPNs, RNs, NPs, the list goes on. You don’t have a doctor who gets a free jet every time they vaccinate a kid. The only “incentive” they receive is a couple hundred bucks that gets taken out for malpractice and/or taxes. Apparently anti-vaxxers still haven’t figured out that the government would give zero fucks as to whether or not pediatricians are getting sued, because it happens all the time already.
The medical industry also wouldn’t be “severely damaged” if we stopped vaccinating. People would be severely damaged. If we were in it for the money, we’d simply give everyone without insurance a C.diff infection. (Just in case you think I’m serious, yes, I’m being facetious). If you think free vaccinations are expensive, you should try paying $1200 for Vanco without insurance. The medical industry would be complete morons for using cheap vaccines as its primary source of money and then giving them to every health worker for free. Saving money is not always an evil plan.
Response: “Do you really think we’re bringing up Wakefield because no one else questioned vaccines, or do you think it’s perhaps because you would willingly spread your asscheeks open for him at any given opportunity after summoning him from the shrine you have hidden somewhere in your home under a pile of turmeric?”
No, don’t actually say that. That would be dealing at an “emotional level” instead of having an argument like a full grown adult.
The reason we would respond “Wakefield’s work was discredited” is because because the anti-vaxxer mentioned his work…. that was discredited. So this doesn’t quite fit into their red herring narrative (not even sure if he knows what that means, considering the amount of red herrings he’s provided so far). But if they didn’t bring him up, don’t do it. They’ll bring him up later, considering the lack of information they have to work with from the start.
When they do so, simply respond with legitimate information about Andrew Wakefield, considering it’s not hard to conclude that the guy is a total shit-bag (they said they like emotional tactics). Unlike all of the other medical fuckups we vehemently despise and mention on a continual basis in every bioethics class, these lovely people keep hailing this particular fraudster as some kind of god-like hero of their campaign. Let me rephrase that: as scientists, we gladly separate ourselves from people who are found guilty of fraudulent data. They don’t get grants anymore. We use them as examples of what not to do in graduate ethics courses. Their name is tarnished. I’m not talking about making a legitimate mistake that leads to a public apology (which would get a paper retracted and some empathetic cringing), I’m talking about the level of disgusting behavior that Wakefield admitted to in court. Like secretly taking blood samples from autistic children from inside of a literal closet without consulting an ethics committee in order to scare parents into paying $43 million dollars a year for a new medical device he patented. But don’t worry, before he joked about illegally taking blood, at least he paid the kids a whole whopping 5 pounds (also illegal- this is essentially pimping). Oh, he also gave them secret colonoscopies and lumbar punctures. Not to mention, he showed no care in the world as to whether or not children were harmed while doing so. On top of that, he deceived his fellow researchers by changing the paper without them even knowing, tearing their names down with him for the purpose of simply having extra names. We bring up Wakefield because there is truly no logical explanation as to why someone would continue to not only support a man admitting to fraud, but deeming him a “whistle-blower” and a hero, and then continue pretend to fight against scientific “bias” and “fraud.” This doesn’t make an ounce of sense, and instead makes one’s entire argument look like it’s built on quicksand. They often assume things about the CDC and evil pediatricians while simultaneously supporting an ex-physician who was found guilty of stealing blood from minors. That is either some serious cognitive dissonance or a serious lack of cognitive functioning that would place the Wakefield-supporter around a 4 on the Glasgow Coma Scale. If that’s the case, please stop fighting with people in vegetative states.
Let’s take a look at this gem again from their response: “remember, when you’re dealing with rhetoric your response must always work at an emotional level which is why the effective responses always take their ‘logic’ and use it against them.”
I don’t know whether I’m more thrown off by the hysterical advice or the rampant solecisms, but it’s hard to imagine a full grown adult wrote that. Regardless, it makes sense now as to why I’ve asked reasonable questions about ingredients or vaccine schedules only to have the anti-vaxxer go off on a random red herring rampage about vaccines being Hitler. Apparently it’s because they’ve been told they’ll win the argument if they scream the loudest and most obnoxiously.
All of their assumptions are completely worthless, considering Andrew Wakefield’s side of the story already came out of his mouth in court, along with a panel of witnesses.
Response: “Really? Show me those studies you supposedly conducted. Because if you actually did do an ‘epidemiological study’ that showed no link between pregnancy and sex, I cannot imagine the hoops your poor innocent math teachers went through to allow you to graduate a single grade, considering a chimpanzee could probably figure that out faster using an abacus than whatever the fuck you tried to do using R.”
While I would applaud him for finally bringing statistics into the equation (no pun intended), what scares me is it seems as if he literally doesn’t know the difference between observing some data on VAERS and typing it out with Real Housewives playing in the background and running a statistics program (possibly with Real Housewives still playing in the background). It wouldn’t take much effort to figure out with a regression analysis (or some binoculars) that sexual intercourse, whether consensually or non-consensually, took place before the pregnancy (aside from a slew of super common “freak accidents” like eye sex explained to me in good old abstinence-only education). Also- You’re not going to get direct causation with running a simple program. Life doesn’t work that way.
But let’s make this hypothetical situation more realistic: if you asked teens in an online survey to report sexual activity before pregnancy, I’m sure more than one of them would claim to be virgin with some kind of miracle birth. This is one reason anti-vaxxers relying off of VAERS is so aggravating. These are not side effects shown to be a direct cause-and-effect of vaccines. But VAERS is continually studied to determine the possibility of serious side effects stemming from of a particular vaccine. This is why we’ve removed certain vaccines in the past. For some strange reason, anti-vaxxers don’t want to take me up on the offer to simply “do the research” themselves using VAERS data and send it in for publication, if they doubt everyone else so much.
As for the null hypotheses mansplain from hell, that made me physically laugh out loud. This poor guy has no idea what a null hypothesis is. Null hypothesis isn’t stuck meaning “isn’t.” to make it [overly] simple, think of it as the opposite of what you’re testing. If you’re testing for two factors being correlated, being unable to reject the null hypothesis means you cannot reject the two factors not being correlated. Of course, treat it like a grain of salt. And of course you can’t accept a null hypothesis, you dumbass.
What’s hysterical is that they’ll sit there and claim any research effectively showing no link between vaccines and autism is bullshit (often without reading the papers) while tossing out the vaccine insert as diehard evidence of causation. From where? Did the space aliens give the “evidence” to us? No, they’re reported in VAERS and studied from the very same data they’re using as a causation Bible, showing no evidence of causation between vaccines and autism.
Not to mention, if it was a giant secret so big that 1/7 of the US could work in healthcare and nobody was able to figure “the truth” except for some random suburban woke folk in California, why would they be able to see it on the first results of a basic Google search without even needing a VPN? These people act as if the super scary government they believe controls everyone has kept a giant secret involving vaccines, but still hasn’t discovered the first page of Google. All inserts are readily available when you simply type the name of the vaccine into a search bar. Why would they provide any of this info to the public if they wanted to hide it?
Observational studies absolutely cannot determine causation. Yet somehow these same people will back up observational studies to “prove” vaccines cause autism (proving is impossible with biological research), and then shit on piles of meta-analyses.
“‘Challenge rechallenge” design with vaccines would get you laughed into oblivion, as it would be a really shitty design for research unless you know a secret way to purge someone’s immunity. Wouldn’t you rather have a study design that actually works?
Response: “I don’t think you know what the word ‘possibly’ means, as you can’t simply claim something is ‘impossible’ without even bothering to elaborate (an ad hominem doesn’t count). That’s not how reality works.”
That’s pretty much all you have to say to this shitty argument until they finally try to explain why it’s somehow “impossible” to have better diagnoses in the 21st century compared to the 19th century.
If anyone thinks his response was actually good, do I really have to explain why it’s fallacious to claim evolving medical diagnoses for the sake of accuracy somehow simultaneously makes all doctors “stupid” in the past, present, and future? Of course the best doctor in 1800 would be eaten alive in a residency program today. I don’t think Orville Wright would know how to fly a jet airplane either, but he was… uh… a tad important in our nation’s flight history. Medicine has dramatically changed in the past hundred years, and we built off of previous discoveries and mistakes alike. Operating theaters used to be literal theaters for shits sake. It took way too long to figure out basic concepts like hand-washing and why it’s bad to throw literal shit on the streets. I feel like a moron unworthy to open a medical textbook every time I show up to school. Most do. We’re not offended by medicine’s past failures. This is exactly why it’s bad to suggest someone should focus on emotional tactics instead of the argument. In his histrionic effort to express his opinions about physicians, he’s indirectly claiming that science is infallible (it’s not) and that medicine should be ashamed of moving forward. They need to focus a tad more on actual vaccine studies and a little less on their obsession with pediatricians, or they end up digging their own graves in the argument.
Nevertheless, the brain is a complex biological organ protected by multiple layers of skin, connective tissue, bone, and dura. They couldn’t study the brain with an fMRI in the 1800s. Even with an extremely difficult neurology class in medical school, we still have so much to learn about the brain, and I assure you that our understanding of autism with still continue to change with our burgeoning research and understanding. Autism is not a disease, and cannot tell someone is autistic by looking at their skin for a rash like you can with someone who has the measles. Even with visible signs, it took us hundreds of years to develop a detailed understanding of vaccine-preventable diseases, not an assumption over a cold beer. Doctors, over a long period of time, compared signs/symptoms with other diseases, developed an understanding of etiology and progression, determined what points they were considered contagious, learned what the pathogen looked like under a microscope, the best stain to use to diagnose, etc. Autism is a wide spectrum of different phenotypes, some of which already have known genotypes and etiologies, that match set of criteria in the DSM-V. It can’t be observed with clinical symptoms and determined with lab results like an infection. Using nuclear magnetic resonance for experimentation would have probably ended in someone getting burned at the stake. You need modern equipment for some modern diagnoses or experiments since electron microscopy, a mass spec, and fMRIs weren’t exactly staple items while Leeuwenhoek was around.
The measles people die from every year. I wish it was “just a childhood illness,” but it killed about 1 million annually just 20 years ago, and about 80K now. And do you know what they had that autistic children have less of? Autopsies. SSPE is easier to diagnose when you have more gross samples.
Anti-vaxxers seem to be the only ones out there who think doctors are some kind of god-like supreme beings who should be able to transcend time and space. I can’t stress enough how weird it is that they continually only focus on physicians out of a slew of other fields that either create, distribute, study, or administer vaccines. I don’t know if they don’t care about other fields, or literally don’t know they exist. We study a ton about vaccines in medical school (unlike what they claim) but the good news is, there are plenty of other fields who study it even more than we do. On top of that, they think pediatricians, the happy-go-lucky personas of the healthcare world, are horrible humans guilty of murder. It’s like thinking Mr. Rogers is a villain; I cannot take these people seriously.
Response: “Bless your little heart.” We’re not giving you vaccine ingredients to replenish some kind of weird body supply of antacid, or you’d be making sense. Instead, when highlighting the safety of the dosages, we’re trying to express that the dosages are safe (dose makes the poison). And when we express that many of the ingredients are already in our bodies, this means that these “scary chemicals” are not so “scary” to your body that is exposed to them on a frequent basis (Aluminum, for instance)- not that the vaccine is already existing in your body somehow. The entire purpose of vaccination is to elicit a natural immune response and subsequent monoclonal antibody production without the infection. The antigen isn’t already in your body or you quite obviously wouldn’t need one. The ingredients in vaccines are not dangerous or in a high enough dose to hurt you.”
Response: (Just face-palm repeatedly)
The difference between blaming anti-vaxxers for spreading disease and not blaming demographics or vague generalizations for spreading disease is substantial.
- Vaccination has nothing to do with sexual orientation, and avoiding vaccination is a choice (assuming there’s no contraindications). Being gay isn’t. On top of it, willingly choosing to put children at risk of disease isn’t comparable to being attracted to the same gender, as gay men are all over the board in terms of life choices and risky behavior (just like heterosexual couples). Some have never had sex, some have it frequently, some use protection, some don’t, some are monogamous, the list goes on. The goal is to encourage safe sex for the sake of prevention. Which we do. With vaccine-preventable diseases, the goal is to encourage prevention as well. I don’t see any hypocrisy in prevention vs prevention.
- IV drug users are an entirely different story. Addiction is a disorder. Being terrified of nonexistent “toxins” in vaccines does not count as an addiction. We do not treat anti-vaxxers and addiction the same way, because they are not remotely the same thing. Someone willingly choosing to be an asshole to everyone around them by putting immunocompromised neighbors at risk of death because vaccine ingredients sound too sciency for their taste isn’t synonymous with someone’s addiction negatively impacting everyone around them. Yeah, addiction sucks. That’s why we’re trying to curb addiction, and are making changes in overprescription of opioids. We can’t just ask people to stop shooting up drugs by simply asking nicely. Anti-vaxxers, on the other hand, have every capability of vaccinating.
- We never encourage people going to the doctor for the sniffles. There is no test for the common cold, and showing up to a doctors office can absolutely transmit infection. This is why we tell people not to do so. If it doesn’t require antibiotics and will blow over, then you can get people sick for no fucking reason. Don’t go to an ER if it’s not life-threatening. We’ve been telling people to avoid doctor’s offices if it’s something that will blow over on its own (but if it needs medical attention, that’s kind of the entire point of going to the doctor), and it’s not our fault this guy was never listening. Don’t go to work and transmit infection, either. I have no idea what this guy is talking about, considering we bitch about gomers on a frequent basis. If you’re sick, stay home from work.

There’s a reason they’re “flinching,” and it’s not because it’s a really good argument. It’s because using his explanation would convince everyone around them that they are homophobic assholes, without ever leading to the magical conclusion this dude is picturing in his head from quixotic daydreams. I’m assuming, even not having very high expectations of anti-vaxxers, that most would completely avoid hinting that all gay men have HIV. The anti-vaccine movement isn’t only one one side of the political spectrum (or you’d find me at the other side), but I’m going to take a wild stab that this dude is a white, cis heterosexual Trump supporter. No reason, just guessing.
Oh, but no worries, he’s totally not homophobic. He’s simply making an argument that makes no logical sense unless you’re really fucking homophobic.
The demographic most impacted by HIV cases are men who have sex with men, and this rate is continually declining with improved sex ed and prophylaxes. They don’t get HIV because they’re gay, instead, they’re simply an at-risk demographic. For example, as a woman I’m more at risk for developing UTIs, and this doesn’t mean my doctor is failing me by not suggesting a sex change. Proper sex ed, which we strongly encourage in the medical field, doesn’t just focus on heterosexual sex. I grew up with abstinence-only education that ignored the existence of LGBT kids in the room and focused only on heterosexual sex in the context of marriage. Instead of pretending it doesn’t exist, any kid needs to know what they’re at risk for (so HIV should be mentioned regardless of sexual orientation), but it’s also really shitty to avoid mentioning to gay teen that protection is important for him as well even if he doesn’t have to worry about pregnancy. This is to encourage safe sex- not heterosexual sex. You’re also not somehow magically protected from HIV because you’re heterosexual. Sex ed should be presented in an informative manner that should never make one ashamed of their sexual orientation, and sexual orientation in itself absolutely does not lead to viruses. In other words, HIV doesn’t pick and choose host based off of sexual attraction – this isn’t Hogwarts (that may not have been in the Harry Potter series either). This guy, however, seems to be confusing CDC data providing at-risk demographics with the medical field encouraging risky behaviors. And that is just downright stupid.
Let me elaborate why it’s stupid. For starters, A PROPHYLAXIS EXISTS. A prophylaxis, just like a vaccine is a prophylaxis, that has substantially reduced transmission of HIV from mother to fetus in developed countries, preventing about 1.6 million children from contracting HIV. It was via that “mad panic” he’s claiming doesn’t exist in the medical community that HIV isn’t a death sentence anymore and kids aren’t watching their moms die only to know they’re next. Instead, individuals with HIV, with medication, can live relatively full lives (~70 years), and nurses who accidentally prick their finger aren’t subsequently writing their wills. We absolutely care about preventing disease and suffering. The difference is that we’re not pointing our fingers at “the homosexuals” and “the promiscuous” like this idiot, which is exactly why we’re moving forward. Take vaccines for example. Instead of of blaming humanity for being viral hosts, we worked to actually prevent the disease. In the meantime, we encourage washing hands, wearing masks when sick, etc. In the case of “the promiscuous” (is he a Baptist minister?), we encourage safe sex. We cannot, however, make safe sex mandatory, and someone’s chlamydia infection isn’t going to transmit the same way as whooping cough.
As the wife of someone who was immunocompromised while receiving infusions for an autoimmune disease that has greatly impacted his life, this guy can go fuck himself repeatedly with a razor bumble ball. Going to the ER was terrifying in terms of keeping him safe from disease, considering some assholes don’t even cover their mouths while over-exaggerating their man flu. He was “actually sick,” and assuming those with autoimmune diseases aren’t actually sick is angering at best. Yeah, I really wish a bunch of people didn’t show up with a simple sprained ankle or the common cold. It was a waste of time and increased his chances of contracting illness. I was pissed about their selfish decisions just like I’m pissed about anti-vaxxers’ selfish decisions. That’s not exactly what I’d call “hypocrisy.”

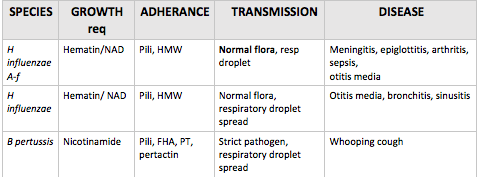
Response: “You are aware that using antigens (like a toxoid) specific to a pathogen is a very basic concept of acellular /subunit vaccination, correct? Did you think that they stuck live contagious bacteria logarithmically growing in a test tube to administer? Our immune system doesn’t have to recognize an entire organism in order for it to be immunogenic. It recognizes patterns and also creates monoclonal antibodies with epitopes against paratopes such as pertussis toxin, filamentous hemagglutinin, and pertactin. Taking this immunological concept into consideration when creating vaccines is what leads to the creation of both IgG and IgM antibodies as well as TCRs against pertussis that have been observed in studies I can provide if you’ll actually read them this time. Overall, immunogenicity against pertussis in those who are vaccinated is quite apparent with serum immunoassays.
Herd immunity, in the case of pertussis, has to be high, but I assure you it exists, although actual peer-reviewed science can provide the evidence for you (you do have to actually read them, though). And due to its need for high herd immunity, quite frankly, I don’t want to be one of the ones contributing to its decrease (I know, I’m scum). And as for asymptomatic carriers, sure, this can be a possibility. But here’s an important part of symptomatic whooping cough: coughing. If a pathogen transmits via respiratory droplets, it’s a tad harder to transmit it when you’re not spraying respiratory droplets all over the place for an extended period of time. And if one keeps up with their vaccinations as an adult, adaptive immunity means that the pathogen will be eradicated much quicker than a primary exposure.

Response: Did you happen to notice how “mainstream medicine” mentioned MMR is not known to shed and according to the actual insert, (“There are no reports of transmission of live attenuated measles or mumps viruses from vaccinees to susceptible contacts“), but the actual diseases can shed or are you so reliant on bullshit that it was actually a concerning factor for you? And how on earth would you get the idea that it’s “just as big a risk as the unvaccinated?” If you haven’t read the package inserts, I would suggest doing so. Too many anti-vaxxers don’t read the inserts
Also, there are multiple stages of infectious disease where one is considered contagious, such as the incubation period and the prodromal period (catarrhal stage in measles). You don’t have multiple periods of infection when “shedding.” I’m not sure why anti-vaxxers use shedding as a “gotcha” point, considering it can only take place with attenuated vaccines, is usually just in feces, and a request to avoid visiting sick relatives the first day one receives a live vaccine, just in case, isn’t “proof” vaccinated kids are spreading the measles. Kids who receive live, attenuated viruses should not visit immunocompromised family members during the first couple of days (which should be common sense), and try not to rub feces on anyone. Unvaccinated kids who actually contracted the measles are like walking petri dishes, contagious off and on repeatedly, even when asymptomatic, including both before and after infection. Stop trying to compare possible shedding of an attenuated version of a virus via poop for a couple days to spreading a highly infectious disease for two weeks.

I don’t think anyone is going to apologize for not “discriminating” against children with Hep B, as it’s not their fault they contracted it. Instead, we’re mad at their parents for willful ignorance. It shouldn’t take a rocket scientist to figure out why we’re pissed people are exposing their children to a deadly virus and potential liver cancer. It is not “hypocritical,” as we’re also definitely “concerned” about those who already have it, which is why there will be a warning on their medical records. But most importantly: you can’t prevent something that has already happened. Why does this guy want us to bully children with HBV because we don’t like people increasing chances of their children getting infected with HBV? What?
The “one in a million or some such” is just a tad important, considering 1/1,000,000 is a much lower chance of death than the mortality rate of vaccine-preventable illnesses. And those who use this guys advice: good luck trying to “illustrate” the cases against vaccine safety by trying to provide evidence for my own field secretly lacking compassion and competency when you’ve never saved a life.

What excuses? My parents lost my recent vaccination records during their divorce, so I ended up getting immunized with both HepA and Gardasil twice before I started medical school. Because Murphy’s law follows me everywhere, I also ended up having to get the two-step PPD twice, because the doctors office closed early on a Monday- the day I was supposed to get my PPD checked the second time. Keep in mind this was two two-step PPDs in the same year I already had a regular PPD that didn’t count. That was five PPD vaccines in one year, six Gardasil shots, and four Hep A shots, plus a quadrivalent flu shot. I have had more vaccines than I was ever supposed to. The only immunization I’m completely missing is chickenpox, because the vaccine was introduced after I contracted it. HepA I received after 1995, though I’m not sure the actual year due to my lost records (I may be a tad bitter). And if this guy thinks the amount in a vaccine is too high for babies, he sure as heck better support that with evidence.
“There are plenty of such stories” Such as, and they don’t have maps and such. “in other words, there is evidence that vaccines cause/trigger autism to a level that would be deemed sufficient proof for any other medication. But not vaccines” No, that’s not how it works. Anecdote is never “sufficient proof” for any medication. And vaccines can be “dechallenged” about as much as you can dechallenge an appendectomy. You can’t get rid of immunity like that without a bone marrow transplant, which would be crappy research to begin with.
I’m also not going to give a kid another vaccine if they had a horrible reaction to the first one. I love it when anti-vaxxers completely go against their own platitudinous rampages about vaccine injuries by specifically stating it’s unscrupulous to not give a child who actually had a reaction another vaccine for a “rechallenge.” We would we want to give them another one if the first one sent them into anaphylactic shock? Anti-vaxxers are such hypocrites. On top of it all, if the reaction was mild (e.g a cutaneous blister) and they got another one the second time they received the vaccine, the physician would send it into VAERS to be used for future research.

This cracks me up for multiple reasons. First, the reasoning and method behind getting the number 500 deserves a Darwin award. Not only is he convinced that a pediatric vaccine approved specifically for pediatric patients somehow shouldn’t be given to a pediatric patients because of dosage, but he determined the dosage by…. uh…. I can’t figure it out. I may have to drink another beer to figure out how he determined someone needs 40 hepatitis vaccines in one day because of how much the average woman weighs in Australia. I’m laughing so hard right now I’m physically crying.
In reality, pretending we were talking about something like Benzodiazapines, here’s an example of what a generic dose equation looks like:

We don’t need this (we couldn’t use it anyways since bioavailability would be impossible), because a vaccine creates an acute localized inflammatory response and isn’t designed to spark a drug response. A vaccine goes off of immunity (an immune response), not drug pathways (an effective level). In other words, it involves your immune cells in a localized part of your body, not your metabolic pathways systemically (or localized in some cases). You’re not slowing down your heart rate like a beta blocker or stimulating your CNS like Adderall. It’s not being metabolized by Cytp450. You just need to create some immunoglobulins for the purpose of memory. Required pediatric vaccines are safe for pediatric patients.
Second of all, ask the person who is trying to debate you what the difference is between DTaP and Td. Hopefully this creates a lightbulb moment as they realize that multiple types of vaccines exist for a reason. You wouldn’t give a kid Td, but you’d give it to an adult – their hypothetical world of different adult and pediatric vaccines already exists.
Third, vaccines go off of a much smaller amount than dosage by weight. Ask them if they’re wanting the amount to be greatly increased based off of weight, or if they’d rather have a one-time IM injection of the enough of the substance to spark an effective immune response. Pneumococcal vaccine has 0.6 mg of alum. In comparison to drug dose by weight, 59 mg Al/mL is what was given daily to patients in clinical trials for the antacid. The LD50 is >5000mg/mL. Now let’s put on our thinking caps: would you rather someone go off of weight and administer a good couple hundred mg of alum, or would you rather have a regular adjuvant that microscopically initiates an immune response? This really isn’t hard. On top of it all, we have clinical trials, VAERS, and meta-analyses for a reason: if one of the ingredients doesn’t work efficiently, isn’t safe, and/or directly causes a plethora of negative reactions, we’ll be able to determine that. That’s exactly how some past vaccines were removed from market in the past and replaced with safer alternatives, such as acellular pertussis. It’s also why we don’t give the anthrax vaccine, the HFM vaccine that’s available in some countries, or the tuberculosis vaccine. If it wasn’t about safety, then we wouldn’t be making active changes for the sake of safety.
He really needs to take some deep breaths. Maybe practice some yoga. I feel like his internal screaming is coming through the monitor. If the person debating you is hyperventilating on the other end to the same extend as this genius, offer them a glass of water or something.
No, nobody is going to take that offer. If they get all hot and flustered or smirk because they think such a dumb question is actually valid, ask them if they drove a car that day. Then ask them if cars work so well, if they would let you willingly allow you to drive over them with it if they’re “so safe.” Then they’ll make lame excuses like “cars don’t work that way.” Yes, this scenario is a red herring, just like his scenario. That’s because we don’t want to inject ridiculous amounts of vaccines because someone else doesn’t understand what a vaccine is or how math works. It’s not an argument. It’s proof that our education system is failing people like this. When he scoffs at “vaccines don’t work that way,” it makes me chuckle to think about the number of people who must have tried over and over again like a broken record to get him to understand that. We can’t help it that vaccines literally don’t work that way. That’s not our problem. I will get 500 vaccines if he is willing to get run over by a schoolbus. And he’s right – nothing we can ever tell them will convince them that vaccines are safe. That’s because they couldn’t give a rats ass about safety. They’re not actually waiting for someone to provide a good enough argument to change our minds like we are, their main argument is to use emotional appeals and use alternative facts to promote a belief system. I’ve had better conversations with Jehovah’s witnesses interrupting a pizza party.
And yeah, the dose still makes the poison. That’s not contradictory – too much of anything can kill you. But the LD50 is >5000mg of just alum alone. If vaccines contained such ridiculous amounts of ingredients, then it would change to a toxicology issue (but hey, it would finally involve weight), not immunology which involves microscopic amounts. The “sheer brazen hypocrisy” doesn’t make any sense, since nothing changed and I’m not backtracking. It’s like this dude has the cognitive reasoning skills of a chimpanzee. The dose makes the poison- that doesn’t change, okay? He used water, so I’ll go off of that- too much water will kill you, But when you look at the back of a juice carton, do you check to see if there’s a lethal amount of water? No, that would be ridiculous. Even if it “sounds nasty” and we pronounced it “dihydrogen monoxide,” it doesn’t change the fact that could could have much higher levels than what is in grape juice concentrate for a toddler or a 45-year-old. Is it starting to click now? The dose isn’t even close to a “critical level.” The difference is that you don’t then adjust the grape juice concentrate to 500 gallons of water for a 45-year-old. This is why math class is important.

Why is Tristan limiting anti-vaxxers to the point where inserts can only be mentioned in the case of “non-inert” placebos, as if that’s a term that’s used in science? Anti-vaxxers tend to get confused between a placebo and a negative/positive control, and they tend to think a saline placebo should be used in an experimental study. Regardless, saline placebos have been used plenty of times to conduct research on vaccines. It helps if you google it. And contrary to what this guy claims, that doesn’t make an ounce of difference when it comes to a discussion about vaccine inserts, but rather contributes to a discussion on the methods used in a specific study. If you’re anti-vaccine, having a serious discussion about inserts and peer-review could potentially lead to a good conversation, as it’s built off of science. As someone who supports vaccines, I’m going to give actual advice on how to debate a pro-vaxxer: if an anti-vaxxer highlights problems they have with a clinical trial or experimental study using methods that would unscrupulously alter their p value, that is one hell of a good conversation. It’s mind-boggling to me that he suggests doing the opposite, because he’s setting anti-vaxxers up for an embarrassing situation by limiting conversations that actually talk about science. Even an anti-vaxxer should be able to see this. What he’s doing is setting anti-vaxxers up to fail a debate every time by making them run off with their tail between their legs whenever studies are mentioned.
It doesn’t make sense to me why he believes vaccine inserts are the “most truthful documents,” since physicians and pharmaceutical reps are the ones who report to VAERS. If you mention this, I’ve always received the response “but they’re underreported!” But that’s not what I’m talking about — that’s another red herring. Regardless of how many injuries are reported, “Big Pharma” is still who is reporting to VAERS and who is publishing stats from VAERS, meaning the negative side effects mentioned are mentioned by whom they deem to be pathological liars. “Big Pharma” is also who is writing vaccine inserts. Anti-vaxxers can’t get around that fact. Either pharmaceuticals are involved in a giant vaccine coverup or they’re not – this isn’t difficult. That’s something you certainly can’t have both ways. And it makes no sense to me why “Big Pharma” would be writing 20+ page vaccine inserts readily available on the first page of Google if they were involved in a giant cover-up. From our point of view, it’s simple: companies write packet inserts to educate and to cover their ass just like most other companies in sue-happy America. Most physicians I know can’t stand pharmaceutical companies. But anti-vaxxers believe vaccine inserts are the “most truthful documents” written by the most “untruthful” people they can imagine, which makes no sense. That’s like a kid in your class stealing other people’s English papers repeatedly and lying about it, but the teacher gives him an A every time she personally agrees with the paper. They’re either pathological liars or they’re not.
When he mentions peer-review, he claims that it will never work because we have hundreds of papers to use in comparison to just a few supporting anti-vaxxers.
This is important!
That’s what “doing your research” looks like – you realize there is way more support on the pro-vaccine than anti-vaccine side. Welcome to the pro-vaccine side, Tristan! Glad you could join us.
Time and time again, as he mentions, meta-analyses support vaccination and anti-vaxxers have a short article here and there until they get retracted. This is when an anti-vaxxer chimes in and says “but anti-vaxxers are silenced!” Let’s pretend they’re right and that only a few anti-vaccine papers get published because Big Pharma is silencing them (or whatever other conspiracy is made up on the spot). This doesn’t explain how fabrication and/or falsification keeps showing up in anti-vaccine articles. Anyone can read for themselves why they were retracted.
But one thing Tristan doesn’t tell his readers (I doubt he knows this) is that you really can have a good conversation about vaccination with less studies on your side if you can support your side well. Yes, they will be at a disadvantage considering the number of papers supporting vaccination, but that’s why I’m serious when I say I support vaccines because I “did my research.” He mentions this briefly and then backtracks, claiming to not even go there. If someone is good with statistics, it shouldn’t be hindered because Tristan is personally bad at math. If someone researched the most frequently quoted pro-vaccine articles and was able to support why the studies were conducted poorly with statistics, they will actually have a great argument on their side. Yes, that’s going to take a ton of time. That’s what “doing your research” looks like. If they follow the advice of Tristan, ask them this: “You’re choosing to have a conversation about vaccines without taking the time to comb through articles supporting vaccination. Why do you think that is?” You can’t make a generalized statement like “so many studies exist” as he’s suggesting without expecting the person you’re debating to ask you about specifics. I’m sure every anti-vaxxer has already experienced this at least once. He gives really horrible advice.

Bingo.
He’s right- we can simply run a regression analysis to support our viewpoint. This is because statistics supports the importance of vaccination. And contrary to what he claims, a regression analysis wouldn’t ever nullify the argument that sex leads to pregnancy, because that’s not how math works. Math isn’t synonymous with opinion. It would support sex leading to pregnancy every single time – because a study like that is reproducible, and we have so much data on that hypothesis that we can further it to determine causation. Often researchers have a link to more data in their study for the sake of curbing any doubt in their results. Someone who later conducts the same study and finds different results can look at their data to compare for the sake of accuracy. Small samples of “choose your own cohort” are actually often found in studies that don’t support vaccination, not support. As an example, there’s a popular study frequently quoted by anti-vaxxers that compares kids who aren’t vaccinated to those who are. This cohort included nothing other than a small sample of homeschooled moms who self-reported how healthy their child was. Talk about biased. Meanwhile, meta-analyses supporting vaccination will take whole countries into consideration over a span of decades. These meta-analyses are then compared to similar other meta-analyses, and similar results are usually found. Which sample are you more likely to accept? N=2,000,000 or N=30? Of course that has meaning. It has a lot of meaning- statistics is one of the most important aspects of the scientific method. People can screw up math (which can be noticed), but math never lies.
A “null result” means it supports the null hypothesis, which may be a positive correlation depending on how their paper was set up.
“Car makers” or food manufacturers also use regression analyses, and why he implies otherwise is beyond me. I don’t he knows what a regression analysis is, which is pretty lazy on his part, considering he has such biased opinions against them. Nevertheless, there aren’t just regression analyses run on vaccines. We have multiple different ANOVAs and both experimental and observational studies. If an anti-vaxxer follows his suggestions, they will look like complete morons.
Why would a CEO need to get behind a car and get smashed into a wall? Why would any reasonable adult think a CEO should do that? If Toyota was able to support with peer-review that their Camry offered more protection from injuries than a Honda Accord, then I’d be more interested in buying a Toyota without wanting the CEO to get their skull crushed in the process. And we have paper after paper supporting that vaccination offers more protection than vaccine-preventable diseases. On top of that, I have received all of my vaccinations, including more that I didn’t need to get like yellow fever. If every person should willingly put themselves at risk to support their opinions, I’d request Tristan get into a room filled with every vaccine preventable disease, which he would obviously (I’m hoping) never do. I wouldn’t request that in anything other than a sarcastic tone because I’m not a fucking sociopath. If an anti-vaxxer asks you to get injected with 500 vaccines because they don’t understand what a “dose” is, don’t realize a majority of the full grown millennials they’re talking to have already received a majority of the same vaccines as infants, and are going on and on about how CEOs need to slam themselves into walls at 100km/hr because they’re drama queens, then ask them to step into a tiny, crowded room filled with deadly diseases. It’s a red herring and makes them come across as angsty teens instead of reasonable adults.
He’s trying to convince his readers that studies aren’t important, but that’s not how reality works. Research is very important. Way more important than N=1 involving one weirdo who wanted to inject themselves with 500 vaccines. That would lead to a case study on the bottom of the “research pyramid,” and would be thrown out on account of 500 vaccines not actually being an “adult dose” of the same shots. An adult shot would be vaccines like shingles and Td. They already exist. The studies are not horseshit, and a biased cohort would most likely be thrown out or at least mentioned as contributing to confounding variables in subsequent meta-analyses.
Well, if you want to show something is useless, I’d probably start by not quoting one source that doesn’t exist.
- The “health of children” is a generalized statement that needs further clarification. Does he mean survivors of sexual assault with PTSD? Does he mean children who succumbed to vaccine-preventable diseases? Does he mean children who were involved in motor vehicle accidents? Does he mean congenital disorders? “Health” needs to be explained. Because children are definitely more protected from vaccine-preventable diseases.
- No. Very detailed books on every possible side effect to vaccination have already done this. We can look at both a reaction-base or an overall trend. If we look at reactions, here’s one for the measles showing quite a significant difference between reactions from the vaccine and reactions from the diease:
Table 5
A comparison of the estimated risks of adverse reactions after measles immunization with the complication rates of natural measles
|
Adverse reaction
|
Measles complication rates per 100 000 cases
|
Adverse reaction rates per 100 000 vaccines
|
Background illness rate per 100 000
|
|
Encephalopathy/encephalitis
|
50–400
|
0.1
|
0.1–0.3
|
|
Subacute sclerosing panencephalitis
|
500–2000
|
0.05–0.1
|
–
|
|
Pneumonia
|
3800–7300
|
–
|
–
|
|
Convulsions
|
500–1000
|
0.02–190
|
30
|
|
Death
|
10–10 000
|
0.02–0.3
|
–
|
If we looked at overall trends, we find that vaccination greatly decreases rates of disease and death worldwide. Unless he thinks death and disease have nothing to do with health, yes, vaccines have improved health. They’re not supposed to cure heart disease and diabetes, they’re supposed to prevent certain diseases
- Diseases were not renamed after vaccination. I have no idea what conspiracy site he got that information from, but it’s right up there with chem trails and flat earth. I had the pleasure of interacting with his twitter, and he kept getting angry and flustered when people described to him very simply how we can differentiate between diseases, trying to prove how they’ve been renamed because serology didn’t exist back in the day. I’m not shitting you, he thought this was a brilliant response.
- Doctors are not, and never have been, instructed to avoid diagnosing vaccine-preventable diseases in a vaccinated child. I can speak from experience in just the first year of med school alone. This was another one his twitter account has obsessed with. Every time I’d explain to him how it worked, it was like talking to a broken record.
- A child who is hospitalized for a condition won’t have their vaccination records at the hospital, as EPIC (electronic medical records) doesn’t automatically pull up their Hx from their pediatrician. That’s way too convenient and easy for something related to EPIC. If we needed vaccination records, we’d have to call their pediatrician’s office and have them fax it.
- In an emergency situation in the case of a vaccine-preventable illness, vaccination status means jack shit. It doesn’t matter whether or not someone tried to prevent it once, what matters is making sure they don’t die now that they have it. If someone came in with measles pneumonia, it’s certainly a zebra, but we’d have to make sure we take care of the pneumonia before we ask questions about vaccination.
- A parent may be asked “has your child been vaccinated against [condition]?” if it’s part of the Ddx. Rarely will you see that a vaccine-preventable disease like the measles or mumps in a vaccinated child, and saying “no, my child didn’t get MMR” may help us diagnose the condition quicker by highlighting it as the most probable diagnosis in relation to both their symptoms and vulnerability. However, we’ll ask this after we ruled it as the condition as well. That’s because we need to bring this up for the purpose of education and an accurate medical record at that hospital, not to completely rule out a vaccine-preventable disease. A vaccinated child will still get tested for the condition. They’re just less likely to have it compared to an unvaccinated child. On top of it, we’re well aware that most stereotypical anti-vaxx moms will lie repeatedly when asked about whether or not their child is vaccinated. Asking about vaccination history of a pediatric patient can be fabricated and doesn’t alter Ddx.
- We are well aware that vaccines don’t work 100% of the time. But they usually work over 90% of the time in those who are not immunocompromised. This greatly reduces one’s chances of contracting a condition, but doesn’t make it an impossibility. Someone presenting with signs and symptoms of a condition will be tested for that condition and treated for that condition regardless of vaccination status.
Ask them:
- Ask them if ~1950s is the year they first used for their regression analysis, and ask them to support that it is the year for “widespread use” according to peer-reviewed science. You’ll win this 100% of the time, because Tristan has explicitly told his followers to never mention either peer review or regression analyses. Because of this, try to bring up peer review as much as possible, not only to be more accurate, but because it’s funny when the vein on their forehead keeps growing from trying to prevaricate.
- Ask them how the flying fuckity fuck these disabilities, most of which have defined etiologies, involve vaccination. Ask them if they actually think blaming vaccines on car accidents is a valid argument, and give them the phone number for a local community college to take some English classes. If they persist, ask them how it’s not because of increasing rates of essential oils, and if they’d like to get back to the discussion.
- Let them know that a (probably his) wordpress doesn’t count as legitimate data. My wordpress doesn’t count as legitimate data either. Data counts as data.
- Deaths fell from smallpox and polio because of burgeoning modern medicine. The same modern medicine he thinks is evil. Amazingly, deaths dropped when the iron lung came out… wow, who would have thought? What we care about is incidence, which decreased dramatically (you have to use the real stats without data from ten years missing like the graphs he provides). The other diseases don’t have vaccines for them, because they’re either not as dangerous, cannot have a vaccine made, or had too many side effects.
Say:
- “No. The purpose of the polio vaccine was to reduce the incidence of POLIO. It not only worked significantly, but decreased the rate of polio by 99% throughout the world, and 100% in developed countries.” Then maybe show them the plethora of etiologies that can cause “non-trauma” paralysis.
Separated by WHO region:

Separated by country:

On top of it, he’s not accurate with describing “it failed” even if we took every account of paralysis into equation, as if the rates are steeply increasing. First of all, it’s pretty hard to find a study that looks at all cases of non-traumatic paralysis over an extended period of time in the first place, considering there’s such a wide variety of etiologies. Studies like [PW New & V Sundararajan et al 2008 or McKinley et al. 1999] provide statistics that show these rates increasing and decreasing throughout decades, and varying according to ethnicity, gender, and location. Recent research points to non-traumatic spinal cord injuries, while we don’t see it now, most likely increasing in the next few decades, and do you want to know why that is? Baby boomers are now getting older. Bones start to wear down with age, and no, that doesn’t count as “traumatic.” That’s non-traumatic. Regardless, the polio-induced cases of paralysis have diminished to almost negligible levels.
- “No. The purpose of the rubella vaccine was to decrease the incidence of RUBELLA” Vaccines are not rocket science. This is the second vaccine in a row he got completely wrong. If Tristan doesn’t know the easiest explain-it-like-I’m-five reasons as to why we vaccinate, then no wonder he’s so confused. Rubella is just one ToRCHeS infection. There are multiple teratogenic pathogens and drugs, and congenital defects are often caused by genetics alone. No, we do not vaccinate against rubella to decrease the overall rate of congenital defects, but one of the many causes. Which is exactly what happened.
- “No. The purpose of the measles vaccine was to decrease the total incidence of measles infections.” Which is exactly what happened. This subsequently decreased the rates of measles pneumonia, measles encephalitis, and SSPE.
- “No. The purpose of the HBV vaccine is to reduce the incidence of hepatitis B.” There are many, many different etiologies of liver cancer. Most often, it’s caused by alcoholism. It did reduce the rates of liver cancer caused specifically by hepatitis B.”
- “The purpose of Hib and Prevnar is to decrease the rate of infections caused by strains of Haemophilus influenzae with the B capsular antigen virulence factor, and the purpose of Prevnar is to decrease the rate of infections caused by specific serotypes of Streptococcus pneumonia.” Which is exactly what fucking happened. These aren’t even the same bacteria! There are multiple etiologies of meningitis and multiple etiologies of pneumonia. Hib and pneumococcal pneumonia don’t usually lead to the same type of pneumonia, either. Hib usually leads to bronchopneumonia and pneumococcal pneumonia usually leads to lobar pneumonia.
- Diphtheria and pertussis vaccines are administered to reduce the incidence of … wait for it….. diphtheria and pertussis. Which is exactly what fucking happened. These are also two completely different pathogens that lead to completely different respiratory infections. Notice there’s no rhinovirus vaccine. Considering that’s the most common cause of URIs, that’s a tad important.
- The purpose of the mumps vaccine was to decrease the incidence of mumps. Which is exactly what fucking happened
I cannot think of a more ridiculous way to highlight problems with vaccination than to completely fuck up the reason behind literally every single vaccine that’s mentioned. I have not read something that cringe-worthy in a long time.cause of “shedding,” yet somehow they’re also simultaneously not getting diagnosed with it because of bias? Right….. maybe there’s another dimension involved?

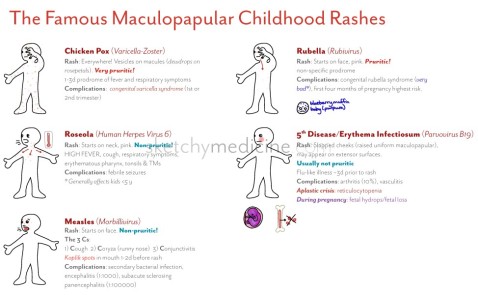

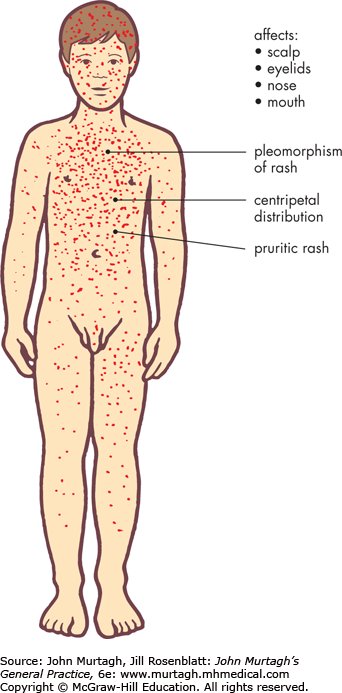






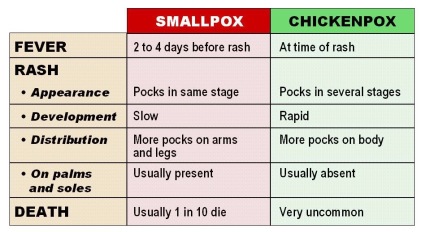
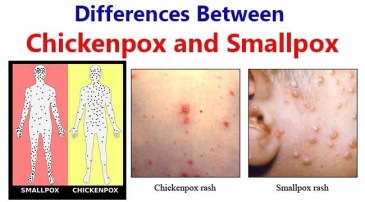 Not the same characteristic rash, not the same clinical presentation, not even the same virus family. In smallpox, lesions begin on the face and then spread outwardly to the extremities, and all lesions will be in the same stage of development. The rash begins at the scalp and head and spreads to involve the trunk and extremities, and the pustules will be at all different stages.
Not the same characteristic rash, not the same clinical presentation, not even the same virus family. In smallpox, lesions begin on the face and then spread outwardly to the extremities, and all lesions will be in the same stage of development. The rash begins at the scalp and head and spreads to involve the trunk and extremities, and the pustules will be at all different stages.